When the US Department of Health and Human Services (HHS) and the Centres for Disease Control and Prevention (CDC) were directed late last year to review and update the US Childhood Immunisation Schedule, professional healthcare bodies reacted with alarm.
Many feared the memorandum would further jeopardise already declining vaccination rates and undermine efforts to protect against vaccine-preventable diseases.
The direction comes in the wake of growing concerns about the sheer number of vaccines on the schedule, the strength of supporting evidence, and falling uptake – a clear sign of eroding public trust.
‘President Trump directed us to examine how other developed nations protect their children and to take action if they are doing better,’ said HHS Secretary Robert F. Kennedy Jr.
In response, the HHS undertook an extensive review of twenty comparable developed nations, analysing their childhood vaccination schedules and the evidence underpinning them.
On January 6, the CDC released its updated childhood immunisation schedule, accompanied by an assessment report and decision memo explaining the rationale for the recommended changes.
These documents, containing the most up-to-date analysis of vaccination practices across the 20 peer nations, highlight several concerning trends with implications not only for the United States but also for Australia.
‘The assessment … found that the US is a global outlier among developed nations,’ the HHS concluded.
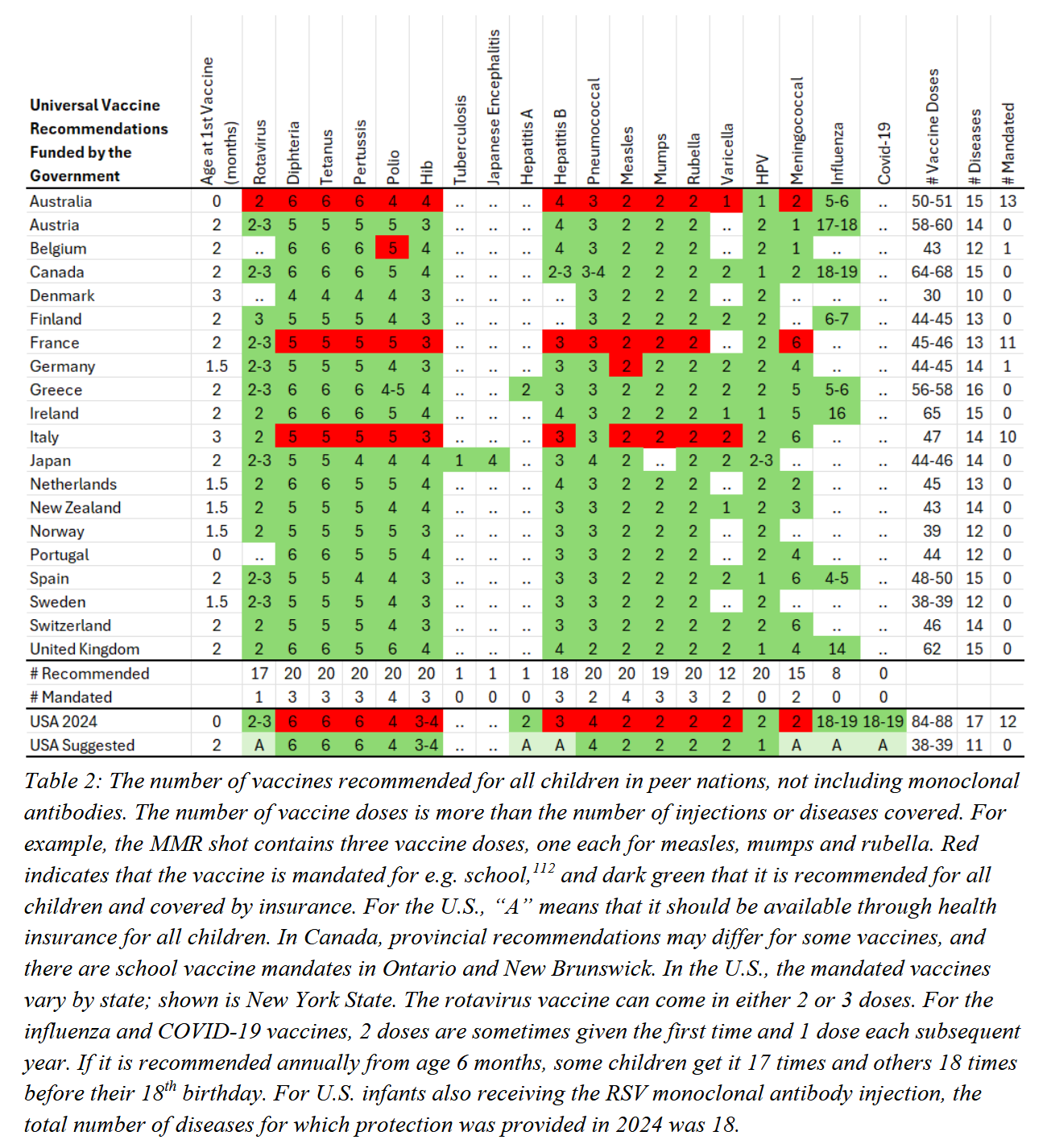
But in what way is it an outlier? When compared with the twenty peer nations reviewed, the United States was found to recommend more childhood vaccine doses than any other country – 84 to 88 in total – and almost twice as many as several European nations. By contrast, Italy recommends 47 doses, France 46, Switzerland 46, Germany 45, Finland 45, Netherlands 45, Belgium 43, Norway 39, and Denmark 30. Australia ranks seventh highest, with 50 – 51 recommended doses, sitting behind Canada (64-68) and the United Kingdom (62).
But more is not necessarily better. As the HHS acknowledges, ‘Many peer nations that recommend fewer routine vaccines achieve strong child health and maintain high vaccination rates.’
For example, while the United States vaccinates against 17 diseases using 84 – 88 doses, many other countries cover 15 – 16 diseases with significantly fewer injections – often between 48 and 65 doses.
The assessment also acknowledged a sharp decline in public trust in US health care institutions between 2020 and 2024, falling from 72 per cent to 40 per cent. This loss of confidence coincided with school closures, other lockdowns, mandatory face masks, Covid-19 vaccination mandates with their de facto denial of infection-acquired immunity, and other public health recommendations that lacked scientific rationale and went against basic principles of public health. The resulting distrust in public health agencies, it noted, has spilled over into attitudes toward other health recommendations, including routine childhood vaccines.
Over the next four years, this collapse in trust contributed to a fall in childhood measles, mumps, and rubella (MMR) vaccination coverage, dropping from 95.2 per cent to 92.7 per cent. By 2025, sixteen US states recorded MMR vaccination rates below 90 per cent – under the critical threshold required to maintain herd immunity against measles.
The US Administration makes a stark admission on the damage pandemic policy inflicted on public trust. It notes, the ‘unscientific belief that vaccine-acquired immunity was superior to infection-acquired immunity, combined with inaccurate CDC claims that the Covid-19 vaccine would prevent infection and transmission, eroded public trust in the Covid-19 vaccine’.
In plain terms: when authorities mislead the public, people naturally start questioning everything else they’re told.
‘Public health works only when people trust it,’ explains FDA Commissioner Dr Marty Makary, signalling that change is needed if public health policy is to serve its purpose. ‘That trust depends on transparency, rigorous science, and respect for families.’
If falling immunisation rates are a barometer of public trust in health institutions, then Australia is in serious trouble. After reaching record highs early in the pandemic, routine childhood vaccination rates are now in steady decline – and the trend is widely recognised.
‘Urgent action is needed to tackle declining immunisation rates,’ declares the AMA.
The ABC likewise reports ‘eroding trust contributing to decline in childhood vaccination rates’.
And Professor Margie Danchin from the Murdoch Children’s Research Institute concedes, ‘Sadly, we’ve actually seen a decline in childhood vaccination rates every year for the last five years through Covid … our rates [are] now at the lowest point in about a decade.’
Yet unlike the United States, which openly acknowledges the role of poor policy and damaged trust, Australian experts have been far more reluctant to look inward. Instead, they have been quick to blame ‘anti-vaxxers’, ‘misinformation’, and – somewhat conveniently – the influence of the Trump administration.
But the decline is real, and it is persistent. Historical data shows that vaccination coverage among Australian children aged 1, 2, and 5 has been falling since 2021: from 94.85, 92.60 and 95.09 per cent in 2021, to 92.14, 90.44 and 93.63 per cent in 2024 – a drop remarkably similar to that seen in the US.
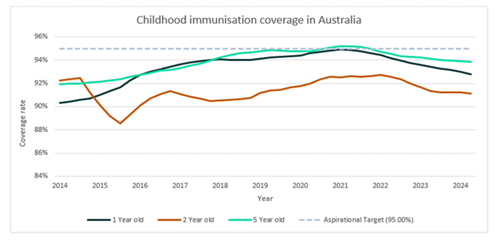
(Source: National Immunisation Strategy for Australia 2025-2030 )
That Australia’s childhood vaccination rates are now at their lowest point since 2015 should be prompting serious reflection from politicians and policymakers. Why? Because in 2015 Australia passed the No Jab, No Pay Bill, introducing financial penalties for parents whose children were not fully immunised. These mandates came into effect on 1 January 2016 and were intended to lift childhood vaccination rates. They did – slightly – over the next five years, until the policy envelope was pushed just a little too far.
It is widely recognised that vaccine mandates carry a risk of fuelling anti-vaccine sentiment, and the US assessment report did not shy away from this. A 2024 comparison between the US and its peer nations found that countries without vaccine mandates had immunisation rates equal to, and in some cases higher than, those with mandates. On average, vaccination rates in mandated countries sat at 88 per cent, compared with 89 per cent in countries with no mandates. And here, Australia stands out: of the 20 nations reviewed, we have the highest number of mandated childhood vaccines – thirteen in total.
It’s reasonable to ask: has Australia now become the most heavily mandated population in the world?
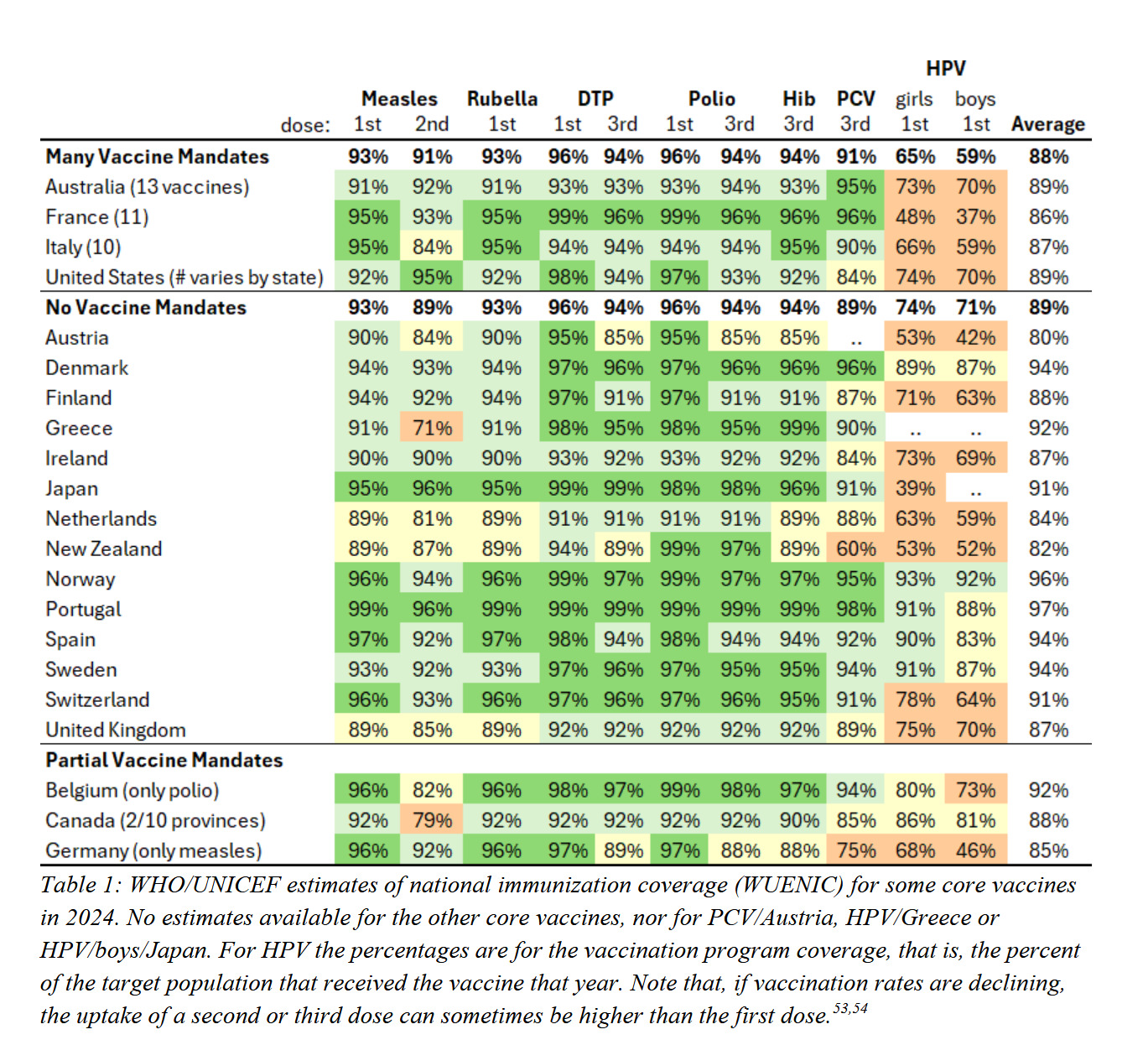
That countries without mandates have, on average, equal – and in some cases slightly better – vaccination rates than those with mandates is an important point to grasp. It suggests that mandates do little to meaningfully increase uptake and, in a low-trust environment, may actually be counterproductive.
The US assessment acknowledges this. ‘While vaccine mandates may increase short-term vaccination rates, coercive measures can also have negative consequences on trust that may decrease long-term vaccination rates for consensus vaccines.’
Which raises an uncomfortable question: are Australia’s chart-topping childhood vaccination mandates now serving to fuel the broken trust in public health?
This is a reality the US administration is no longer prepared to ignore. ‘With a few exceptions, peer nations do not have childhood vaccination mandates. They have shown that transparent and trustworthy public health authorities can achieve very high voluntary vaccination rates while preserving informed consent.’
Instead, the US is deliberately returning to the foundational principles of ethical medical care: self-determination, personal autonomy, and informed consent. As the assessment report explains, a renewed focus on personalised care and shared decision-making strengthens informed consent, improves the doctor-patient relationship, and helps rebuild trust in public health.
And the US is acting on that. ‘After an exhaustive review of the evidence, we are aligning the US childhood vaccine schedule with international consensus while strengthening transparency and informed consent. This decision protects children, respects families, and rebuilds trust in public health.’ The updated schedule still recommends vaccination against ten internationally agreed diseases, but does so with more flexibility, less coercion, and a clear emphasis on informed consent. Time will tell how effective these reforms prove to be – but they are an evidence-based and credible start.
So, what about Australia? With more mandated childhood vaccines than any comparable nation, we are now the outlier. In 2026, Parliament has an opportunity to confront this trust crisis by restoring choice and informed consent through Senator Alex Antic’s No Jab, No Pay (Repeal) Bill, and begin rebuilding confidence in our childhood immunisation program.
The question is: do we have the courage to do it?
Julie Sladden is a former medical doctor and co-director of Australians for Science and Freedom. If you’d like to support her caffeine-inspired writing, you can shout her a coffee here.