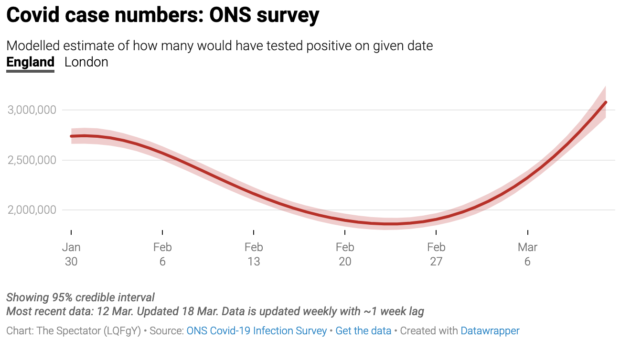
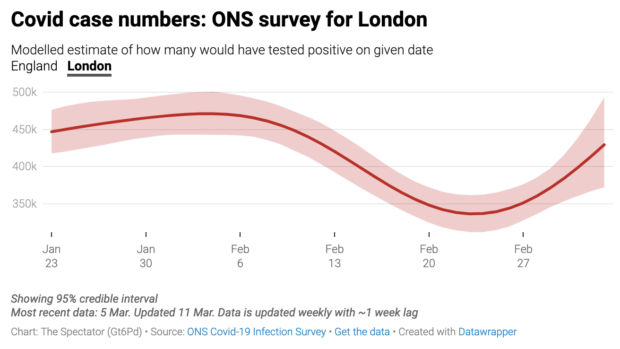
When the Omicron variant (now categorised as BA.1) swept across the world at the end of last year it was seen by optimists as the final chapter in the Covid story – it was so contagious it would infect essentially anyone, but would be far less likely to cause serious illness. Now a new wave of Omicron – the BA.2 variant – is becoming dominant in many parts of the world. In the UK, cases are again on the rise.
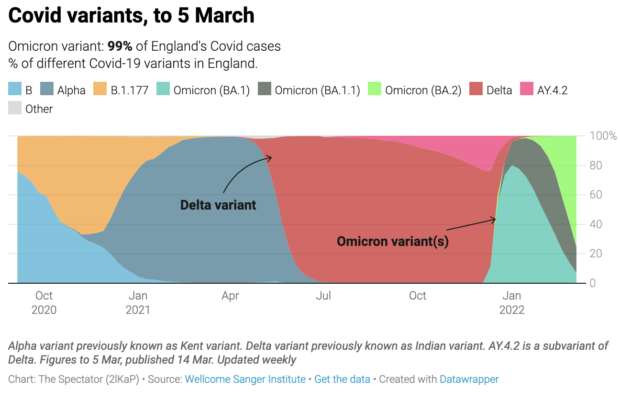
Genomic surveys show that BA.2 made up 76 per cent of new cases in England as of 5 March. The below is from the Sanger Institute:
So what’s going on? Firstly, both the BA.1 and BA.2 variants do not have an intrinsically much higher growth rate than any previous variant. Instead, they have spread globally for two main reasons. First, both can infect people who were protected from earlier viral strains by vaccines and/or previous infection because their spike proteins (the region which neutralising antibodies, which protects people from infection by the virus, bind to) are drastically different to any previous Covid strain.
This means that in terms of protection against infection, even populations with high rates of vaccination or prior infection were essentially encountering it as an almost novel virus.
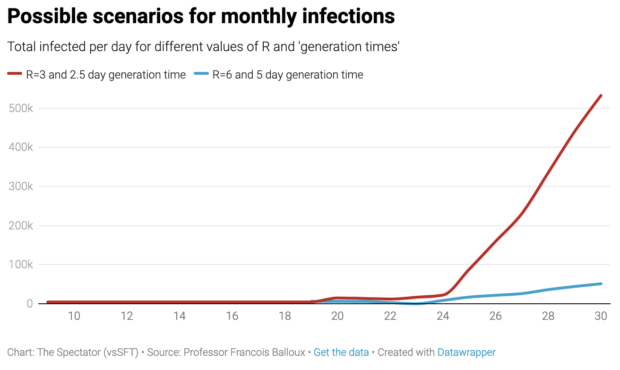
The second reason behind the explosive growth of Omicron is that its incubation time (the time interval between one infection and the next) is much shorter than for any previous Covid lineage. BA.2 has an even shorter incubation time than BA.1.
Shorter incubation can lead to explosive growth in daily case numbers over a short period of time even if each infected person passes on the virus to a similar number of other hosts.
Despite the ability of BA.1 and BA.2 to readily infect and re-infect people, vaccines and prior infections still protect from severe disease and death, thanks to T-cells that cannot be bypassed by the virus as they target hundreds of different sites across the viral genome.
Moreover, contrary to antibodies which are largely identical in different people, each person mounts a unique T-cell response that targets different sites in the viral genome. As such, a virus simply cannot evolve to escape T-cell recognition at the level of the host population.
A lot has been written about Omicron being ‘mild’ (or not). Alpha was around 50 per cent more virulent than the first Covid strain, Delta was again around 50 per cent more virulent than Alpha, while Omicron is around 70 per cent less virulent than Delta.
This means that Omicron is about as ‘mild’ (or severe depending how we look at it) as the original Covid strain we confronted in early 2020, before the Alpha and Delta variants emerged. BA.2 is not more virulent than BA.1.
Being infected with either BA.1 or BA.2 gives you decent immunisation against either variant, but not against pre-Omicron variants. This is to be expected as cross-immunity is largely symmetrical: as pre-Omicron infections give poor protection against Omicron, the reverse must be true as well.
This does not mean though that being infected with either BA.1 or BA.2 won’t protect you against future variants as has been claimed by some.
The recent outbreaks and resurgences of cases in many parts of the world are in part caused by the unique properties of BA.1 and BA.2. For example, the short incubation times of BA.1 (and even more so BA.2) mean that these variants are incredibly difficult to control using test and trace.
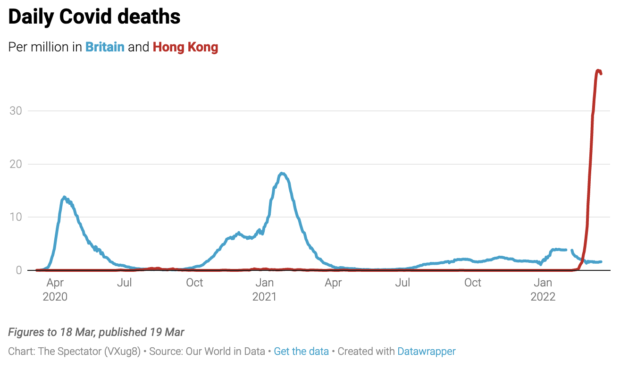
Hong Kong, which had an excellent record in avoiding the worst of previous Covid strains, but an awful vaccination rate among the elderly, is now reporting a Covid mortality rate far higher than Britain saw at any time during the pandemic.
Countries that have good vaccine coverage such as the UK, or that experienced massive numbers of infections in previous Covid-19 waves such as South Africa, remained relatively unscathed during both the Omicron BA.1 and and BA.2 waves.
Epidemic waves can take place for lots of reasons. There are four main drivers: pathogen evolution, seasonality, host immunisation (due to vaccination and prior infection), and peoples’ behaviour (both spontaneous and driven by mitigation measures) that act in concert to drive cases up or down.
It can be difficult to disentangle the contribution of those four forces in epidemic waves. This is particularly the case now, with the ongoing spread of the BA.1 and BA.2 variants coinciding with the lifting of pandemic mitigation measures, and the onset of winter and then of spring.
There is no doubt that Covid is seasonal; all 200 respiratory viruses in circulation are. But this does not mean that it is necessarily most transmissible in the midst of winter. We don’t know yet at what exact time of year Covid will tend to be at peak transmissibility, once it ‘settles in’ into an endemic dynamic.
For example, seasonal flu typically causes one winter wave, and a spring wave each year. The four seasonal endemic coronaviruses in circulation that contribute to 15–30 per cent of common colds tend to peak at different times between winter and late spring.
While the current BA.2 wave, so close on the heels of the Omicron (BA.1) wave might feel like yet another setback, making the pandemic seem like a never-ending nightmare, it has to be put in context. Epidemiologically speaking BA.2 is hardly any different from Omicron (BA.1), with the exception of an even shorter incubation time.
Covid cases are currently going up throughout Europe. This will lead to increased hospitalisations and deaths over coming weeks. Though, about 56% of current Covid hospitalisations in the UK are incidental (i.e. ‘with’ rather than’ for’), and largely reflect the high rate of infections in the community.
BA.2 won’t be the last SARS-CoV-2 variant, but it is far from the worst we’ve experienced, and its toll is expected to be incomparably lower to those of the Alpha and Delta variants.
Pandemics end, messily, and with a whimper rather than a bang. If we’re really lucky, BA.2 may be among the last variants that capture the public’s attention, before ‘viral variantology’ with all its bewildering and arcane terms and concepts again becomes the object of study of professional infectious disease epidemiologists, with the rest of the population largely losing interest, as it should.