Last week, the Therapeutic Goods Administration announced Australia’s second death likely caused by blood clotting from the AstraZeneca vaccine. This took the total reports of cases of the rare and severe blood clotting disorder TTS following the AZ vaccine to 48. But to be attributed to vaccines, the TGA-appointed expert group must determine there is a link. So why haven’t Australian health authorities followed the same careful distinction between dying from and with Covid?
On 10 June, Britain’s National Health Service directed hospitals to change how they record Covid, henceforth differentiating between those seeking treatment for another illness and those actually sick with Covid symptoms. This will help the NHS to evaluate the success of the vaccination program, just like the previous conflation helped to heighten public fear by exaggerating the number of ‘Covid’ deaths.
The United States Center for Disease Control and Prevention is even more brazen. From 1 May, it has explicitly adopted double standards in the PCR tests cycle threshold (below or above 28) for recording a Covid death depending on the vaccination status of the deceased. This will minimise the number of Covid deaths after vaccination but maximise them for the unvaccinated: a curiosity picked up by Judge Richard A. Brueggemann in a judgment on 8 June lifting all Covid restrictions imposed by Kentucky Governor Andy Beshear. An unvaccinated person who tests positive at 40 cycles is recorded as a Covid case despite having no symptoms. A vaccinated person who tests positive at 28 cycles, displays key Covid symptoms but dies at home is not a Covid case because there was no hospitalisation. A third dies in hospital but with a positive PCR test of 29 cycles and is not officially a Covid case. Like Humpty Dumpty, the CDC can make ‘Covid’ mean whatever it chooses to.
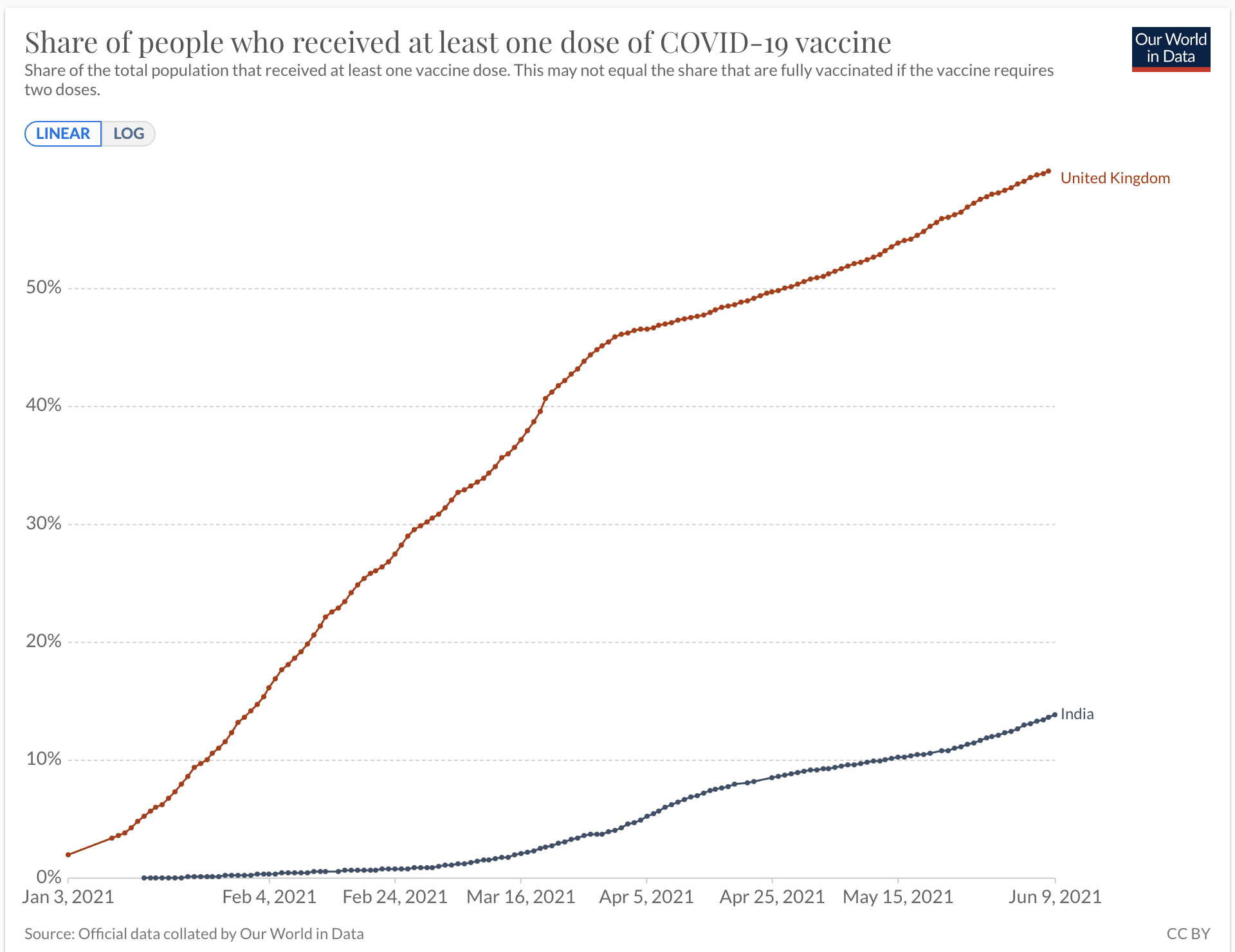
From the start of the pandemic, I’ve been far more focused on observable data than abstract modelling or theoretical speculation. The world-leading success of the UK vaccination campaign impressed with the accompanying steep fall in Covid mortality. The stubborn hesitancy in reopening has been puzzling until I looked at the dramatic surge and fall in India’s Covid metrics. The graphs plot the vaccination penetration of India (low) and the UK (high) and their daily Covid deaths per million on a 7-day rolling average. India’s deaths peaked on 23 May with 10.87% of the population vaccinated; the UK’s on 23 January with 9.36%. But 14 days earlier, around when infections would have begun to decline, their coverage was 9.70% and 3.16%; 17 days after the peak, India (9 June) had increased to 13.86% and the UK (9 February) to 19.24%.
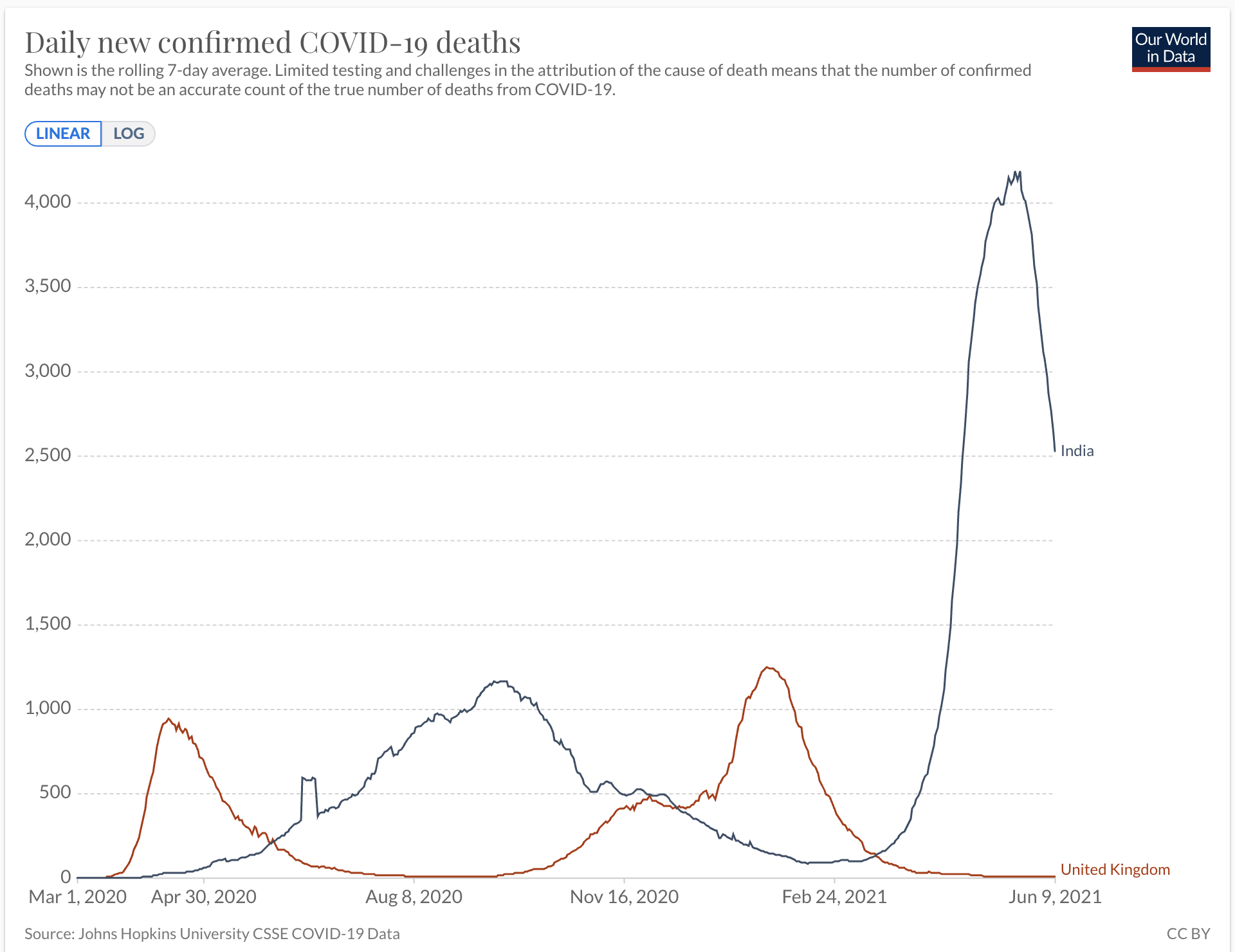
Despite the wide variation in the rate of vaccination (Figure 1), the mortality curves are remarkably similar in the steep ascent and descent (Figure 2). Rather than vaccines, could the steep UK falloff in cases be explained by simple seasonality? Perhaps the UK authorities know this but, rather than confess that vaccines are not the silver bullet that was promised, they will use the excuse of mutant scariants – in this case the Indian variant – to extend lockdown restrictions.
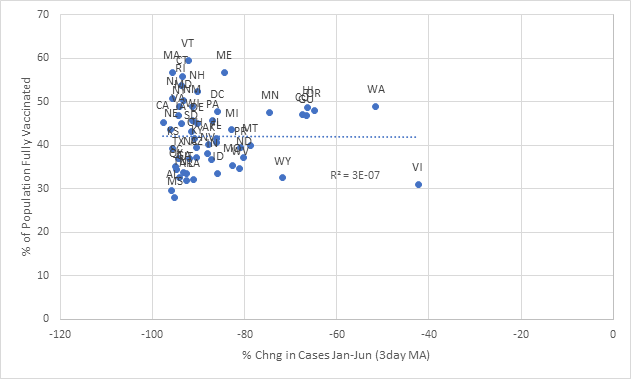
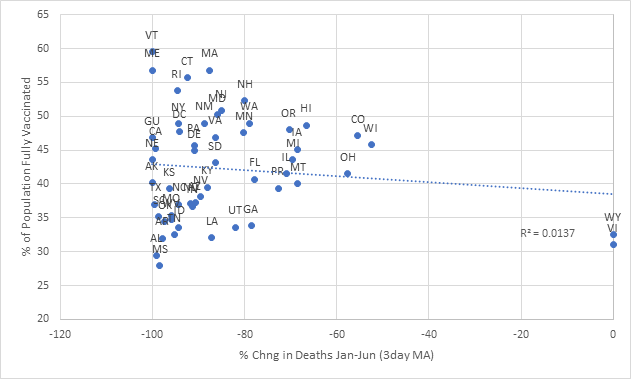
Puzzled, I looked for data on US states. The next two scattergrams, created by an anonymous academic economist, plot the coefficient of determination (a statistical measure that determines how much of the variance in one variable can be explained by another: R squared of 1 is a perfect explanatory ‘fit’) between the percentage of vaccinated Americans and changes in deaths and cases. If the vaccines were having a significant impact, the scatter would be concentrated along a downward sloping line. This is not the case. Rather the scatter is random, meaning there is no detectable impact of the vaccines on the decline in Covid metrics. Something else is causing the decline.
One cause of falling confidence in official assurances is the bait-and-switch tactic of using relative risk reductions to talk up vaccine efficacy, but absolute risk to assuage hesitancy. If my assets total $10,000 and yours $20,000, relative to me you are twice as ‘wealthy’ but in absolute terms neither of us is rich: the relative benchmark is useless in the real world. Among the general public (and for Queensland’s Premier?), much of the vaccine hesitancy stems from awareness of the relative risks of serious side-effects between the AZ and Pfizer vaccines. Health authorities switch to absolute risk measures to reassure and encourage vaccine take-up. A Lancet article gave the relative risk reduction of five vaccines from 67% to 95%, but their absolute risk reduction ranges from 0.84% to 1.3%. Why? Possibly because according to Worldometers, of the currently active 12.6mn cases worldwide, only 0.7% is ‘serious or critical’. A 95% efficacy within a 1% subgroup will not register even as a blip on the mortality curves. CDC data show 4,863 deaths following vaccinations between 14 December and 24 May.
On 1 June, 27 global medical specialists including Australian Professors Peter Collignon and Barbara Mintzes made a formal submission to the FDA that is as sobering as it’s professional. They warn against converting emergency authorisation into general approval for the vaccines ‘until all necessary efficacy and safety studies are completed’ and ‘substantial evidence’ demonstrates that benefits outweigh harms during ‘at least’ two years of further studies, entrusted to people with no conflicts of interest.
Returning to India, seasonality cannot explain the falling curves. The weather was already warm when cases and deaths surged. Moreover, the dominant strain behind the surge was precisely the Indian variant. So what explains the fall? It could just be the natural progression of Covid curves. Or, let’s return to the justification for emergency authorisation of vaccines before trials are completed: the lack of alternative treatments. Significant numbers of specialists have been touting the benefits of preventative and therapeutic treatment by hydroxychloroquine, ivermectin, zinc and azithromycin. Some observers pointing to the use of ivermectin by some Indian states to explain the drop in numbers.
On 25 May, the Indian Bar Association, a Mumbai-based private body, served a legal notice on WHO’s chief scientist for suppressing information on studies that show the efficacy of ivermectin. Studies dismissing them were rushed to publication by influential journals – and some had to be retracted with considerable damage to the reputation for quality and reliability of the journals – while others documenting positive outcomes were cold-shouldered. As we now know in relation to the Wuhan lab-leak possibility, peer review was a proxy for peer pressure and gatekeeping. Ian Birrell points out that publishing houses that own Lancet and Nature are dependent on Chinese financial sponsorship.
Finally, should we continue to ignore the visual correlation between vaccine rollouts and spikes in Covid cases in India, Cambodia, Seychelles, insisting these are all conspiracy theories, nothing to see here, there or anywhere?